CAPABLE Overview
CAPABLE is a client-directed home-based intervention to increase mobility, functionality, and capacity to age in their community for older adults. CAPABLE consists of time-limited services from an occupational therapist, a nurse, and a handy worker working in tandem with the older adult as an inter-professional team. A key component of this approach is having the older person drive the goal setting and brainstorming strategies with the team toward reaching their goals. Each service builds on the others by increasing the participants’ capacity to function at home. This can decrease hospitalization and nursing home stays by improving medication management, problem-solving ability, strength, balance, mobility, nutrition, and home safety, while decreasing isolation, depression, and fall risk.
Participants work with the occupational therapist and nurse to identify three achievable goals per discipline. The team members use motivational interviewing to examine how to overcome barriers to independent living. The participant learns new skills, exercises, and how to work with additional tools/equipment/home modifications-- practicing in between visits. In the case of safe bathing, for example, barriers could include a slippery tub, muscle weakness, and lack of grab bars which impact how to get safely into and out of the tub. In this example, the occupational therapist and client work together on safe ways to use the tub including selecting the proper adaptive equipment, plus ways to conserve their energy. The registered nurse addresses medical or condition related factors that could affect balance, such as pain, and the handy worker makes structural improvements needed to overcome these barriers, such as installing grab bars and repairing broken flooring.
Yes. CAPABLE is approved by the National Council on Aging as an evidence based fall prevention program. CAPABLE has been tested in multiple small and large trials each showing a benefit towards better function and lower hospitalization rates. The larger studies have also showed decreased nursing home admission. CAPABLE is being recognized by Federal and State agencies as an effective program in improving health and decreasing costs among older adults. Click here for a live map of CAPABLE locations.
Generally, in 10,000 people over 65, 40%-50% will have difficulty with at least one Activity of Daily Living (ADL). After subtracting the 10% who have dementia, there should be approximately 3,500 who can benefit from CAPABLE. This will, of course, depend on the composition and characteristics of your own population.
Program Implementation
To adopt the program, the organization(s) will need to identify and address the following at a minimum:
- Capacity, staff resources, workflow, and where the program will be “housed” within the organization(s)
- Training of the registered nurse (RN) and occupational therapist (OT), program administrator and identification and preparation of the handy worker services to be engaged
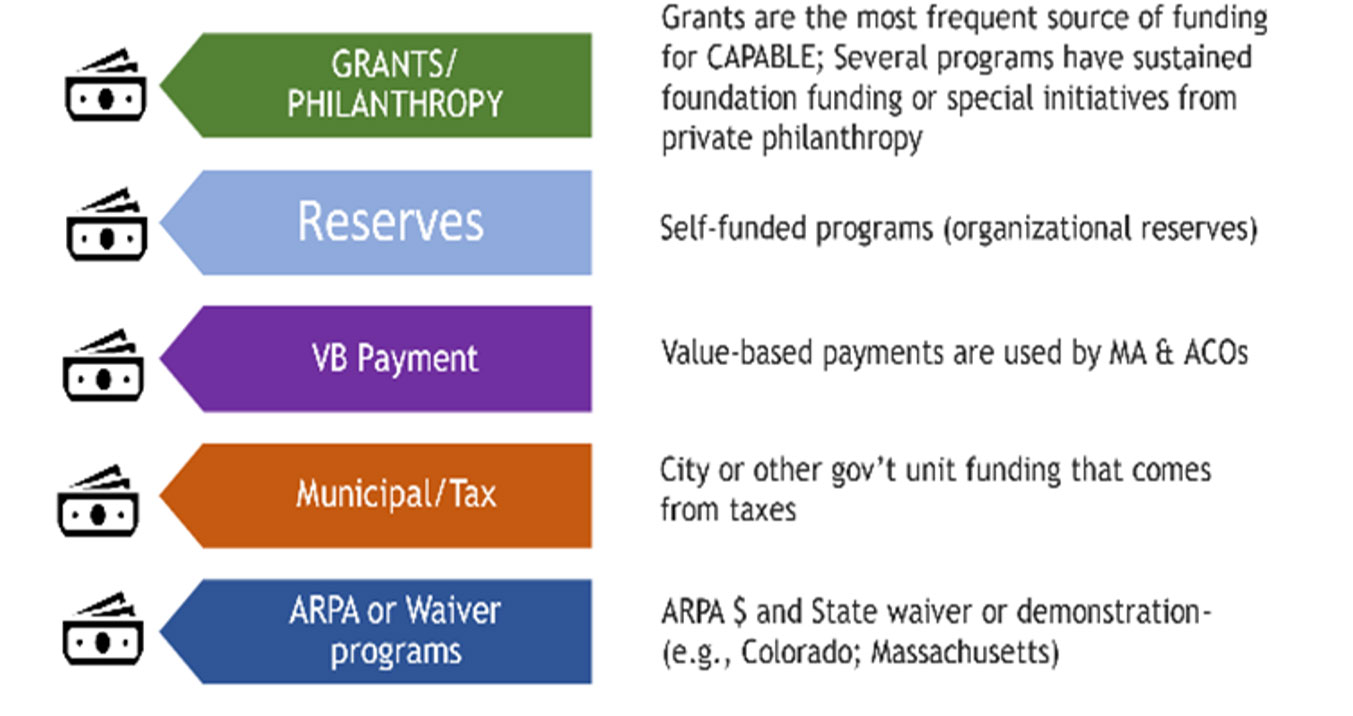
- Funding for the program with an eye towards a sustainable business model
- How the program will be monitored and evaluated
With regard to the flow of the program, these are the key components and steps:
- Contact CAPABLE National Center for information and guidance/Technical assistance
- Complete CAPABLE New Site Information request form
- Determine lead organization, key contact and/or program administrator
- Determine partnership or single organization approach – ensure leadership commitment
- Review CAPABLE protocol and Fidelity expectations
- Identify and secure start-up funding
- Create plan for initial implementation that matches capacity and funding
- Sign licensure agreement with Care Synergy CAPABLE National Center
- Set measurements/results/goals
- Hire/contract staff
- Train clinical staff through Care Synergy CAPABLE National Center
- Begin invitational/referral/marketing strategy
- Follow protocol and serve participants
- Participate in continuous learning/sharing with CAPABLE National Center team and CAPABLE community
- Provide annual survey of results to CAPABLE National Center
Visit Series
- Initial Screening and Interview
- 1st OT visit – includes assessment and discussion of priority goals
- 2nd OT visit – includes fall prevention and recovery, examining the home and working with the participant to create a goal-related work order for the handy worker
- Handy worker comes to make repairs and accessibility modifications. A site visit maybe necessary to assess for needed supplies to do the work
- 1st RN visit focuses on pain, strength, medication, communication with health care providers, set goals
- Additional OT visits to address priority goals and develop/complete action plans
- 2nd RN visit - includes review of CAPABLE exercises, consider how to improve communication with primary care provider, develop action plans
- Additional RN visits to review progress and use strategies, complete action plans
- The final RN and OT visits are a wrap-up and help the participant generalize what they learned so that they can address new challenges.
Many types of organizations are implementing CAPABLE. This includes: health care systems, Accountable Care Organizations, Area Agencies on Aging, Medicare Advantage health plans, insurance companies, PACE programs, state/county/city Department of Aging, Home and Community Based Services providers, skilled nursing facilities, nursing homes, Veterans Administration centers, home healthcare agencies, and non-profit organization in the healthcare and housing sectors. There is also potential for local startups to offer CAPABLE as a self-pay model.
No, CAPABLE can be implemented anywhere older adults live.
- Private homes, condos, townhomes (pursuant to association rules)
- With clearance from the landlord:
- Apartment buildings
- Other non-home owner situations (e.g., participant lives in a relative’s home)
Organizations generally determine participant eligibility criteria that fit the needs of their location. The evidence base of CAPABLE is with people who:
- Are older adults (over 60); although some health systems are recruting people as young as 18.
- Are cognitively intact or have only mild cognitive impairment to be able to participate in the brainstorming and action planning process.
- Have some or a lot of difficulty in performing Activities of Daily Living (ADLs), such as bathing, dressing, grooming, or walking across a small room. This could apply to adults at any age with ADL difficulty.
There are several possible sources for a handy worker. For instance, we have worked with an AmeriCorps training site that trains handy people to do such work. Other possibilities include:
- Hire one internally
- Contract with an AmeriCorps training site or a non-profit home modification organization
- Contract with one of the many companies that provide home modifications for older adults
- Utilize Lowes Livable Home
Knowledge and experience with local code requirements is advantageous. There currently is no specific CAPABLE National Center training for the handy worker, however we do conduct quarterly office hours for the handy worker. There is also a brief video available for viewing as part of the training for clinicians that describes the CAPABLE Handy worker experience. We require orientation on the CAPABLE program, and basic skills in working with older adults, as well as background check and other organizational clearances per your state (licensed, bonded, etc.) to ensure the individual has the necessary credentials and does not pose a risk to the older adult.
Environmental changes at home; decreasing falls hazards, improving balance, improving strength and mobility; reviewing medications and potential need for changes in working with the prescribing physician; providing self-care strategies for better management at home. Participants have also raised issues around incontinence/bladder control, fatigue, muscle weakness or stiffness, poor vision, and social isolation. Examples of approaches or strategies that have been helpful including showering later in the day when the body is less stiff to increase ease of bathing; identifying specific products like LED lights or medication reminder alarms. All services support achieving the participant-identified goals.
The occupational therapist works together with the older adult to determine what will be modified. This is based on the participants’ goals for meaningful daily activities. The handy worker may also add basic safety repairs after consultation with the OT and budget allows.
Here are examples of each.
Modifications:
- Install grab bars in the tub area
- Install interior and/or exterior railings
Repairs:
- Fix hole in floor
- Staple down loose wall-to-wall carpet
Medical equipment:
- Tub transfer bench
- Raised toilet seat
Everyday items:
- Night light for safe transfer from bedroom to bathroom at night
- Sturdy step stool with a rail to reach kitchen cabinets safely
Training & Staffing
Yes. Registered Nurses and Occupational Therapists are required to be trained through the program developed by Johns Hopkins School Of Nursing called the Hopkins CAPABLE training program, which consists of the following activities:
- Reading the discipline specific training manuals
- Seven 60 minute on-line learning modules (self-paced)
- Completing the CAPABLE Home Visit Simulations (OTs and RNs have access to both discipline simulations. Encouraged to review both.)
- Office Hours to ask questions, brainstorm ideas, share successes
- View videos on specific subject matters and client sessions
Occupational therapists can receive American Occupational Therapy Association (AOTA) approved credits for completing the CAPABLE OT training program through the CAPABLE National Center. This is currently possible through the contract with The Johns Hopkins School of Nursing which is an AOTA Approved Provider of professional development. PD activity approval ID# 11558. This intermediate level training is an independent distance learning OT Service delivery course. Upon completion of the curriculum the learner is awarded 1.0 CEUs or 10 contact hours. The assignment of AOTA CEUs does not imply endorsement of specific course content, products, or clinical procedures by AOTA or indicate AOTA approval of a certification or other professional recognition.
Registered nurses can receive American Nurses Credentialing Center’s (ANCC) Commission on Accreditation contact hours for completing the CAPABLE RN training program through the CAPABLE National Center. The courses are provided by the Institute for Johns Hopkins Nursing (PO103) which is an ANCC accredited provider of nursing continuing professional development. Upon completion of the curriculum, the learner is awarded 10 contact hours. Upon completion of the curriculum, the learner is awarded 10 contact hours.
The training for CAPABLE provides team members training in motivational interviewing skills. They use these to build the self-efficacy of the older adults who have functional difficulty. While the older adult is in charge of what the goals are, the Registered Nurse and Occupational Therapist use their clinical knowledge and experience to support the older adult’s goals through a process of brain storming and action planning. This is crucial. These skills require critical thinking and experience in working with older adults in their own homes. One year of experience as a clinician is recommended
The occupational therapist (OT) and registered nurse (RN) can not be substituted and have the program still be called CAPABLE. The training builds from the knowledge base and experience of occupational therapists and registered nurses. For instance, building from the education in occupational therapy, the focus is specifically about activity analysis and achieving the best fit between persons and their living environments to maximize daily function and home safety, and reduce difficulties with Activities of Daily Living (ADLs). The nurses use their pathophysiological knowledge in addressing pain, mood, and medication complexity. The critical thinking involved builds on how OTs and RNs are trained.
Social work can be added as an addition to CAPABLE very successfully. This is especially useful in situations with complicated family dynamics or when access to benefits and other resources are needed. This does not take the place of the occupational therapist (OT) and registered nurse (RN).
We have added the role of the Care Partner Support Specialist which can be filled by the social worker. Their function is to support the care partner in a person-centered approach that benefits them as well as the CAPABLE participant.
No they do not. The clinical team members are enrolled in their discipline specific training track. They complete the self-paced modules on their own. There is an opportunity for the nurses and occupational therapists to access the others' simulation component in the online training. Doing this helps build an appreciation for the other's role in CAPABLE.
One full time Registered Nurse (RN) and one full time Occupational Therapist (OT) dedicated to client visits only, can carry a caseload of 30-35 at a time which leads to seeing up to 100 clients in a year.
Yes. CAPABLE is a pre-emptive, proactive, health promotion, behavior and environment change program. It focuses on both the person and their environment, through a structured, time-limited series of interactions with the inter-professional team of OT, RN, and handy worker--with the participant--not a doctor--dictating goals and action plans.
CAPABLE is not "medical". CAPABLE is not a substitute for physical or occupational therapy or nurse home health care visits, as directed by a physician or nurse practitioner who may prescribe such therapy and home visits--for example after surgery. In fact, sometimes the CAPABLE occupational therapist or nurse refer people for home health visits by an occupational therapist or physical therapist.
Cost Considerations
Email CAPABLEinfo@capablenationalcenter.org for further information.
The cost for providing CAPABLE per person is approximately $3,000 - $5,000 over a five month period.
This average cost includes:
- Registered Nurse and Occupational Therapist salaries, including home visits, driving time, coordination, follow-up
- Mileage reimbursement to/from the home visits (may vary widely by region)
- Home repair, modification, assistive equipment, and everyday items. It is crucial that the system be able to pay for items needed to help older adults reach their self-identified functional goals and enhance their home safety that are not normally deemed “medically necessary” such as a sturdy chair with armrests, a mailbox, or loud doorbell.
- Supervision meetings
These did not include the tablets for data collection or Electronic Health Record (EHR) modification.
Sample start up budget available upon request.
Not yet. This is a work in progress. In June 2019, a committee that advises the Government approved CAPABLE to be considered for reimbursement by Medicare. There will be many next steps. In the meantime, Accountable Care organizations, insurers and other organizations that can benefit from reducing hospitalization or nursing home admission are potential payers or partners.
Program Support
- Implementation manual
- Training manuals for the Registered Nurse and Occupational Therapist *
- C-CAP assessment forms *
- Documentation forms for home visits*
- Brainstorming, and action planning forms*
- CAPABLE Exercise Booklet, Health Passport, medication calendar, Tip Booklet, and items for the participants folders*
- Office hours so trained clinicians, as well as program administrators, and construction partners can ask questions, discuss challenging cases, share equipment solutions, and participant successes.
- Each OT can have up to 3 work orders reviewed.
- Access to Vimeo video clips of visit scenarios
- Access to other CAPABLE sites’ outcomes and experience through an online user group.
- * These materials will be supplied electronically. The cost of copying is the responsibility of each organization
Every organization develops their own system that best works for their staff. Some CAPABLE programs use:
- In-person or virtual coordination meetings
- Emails
- Phone calls
- Electronic health record platforms and data systems that can support interprofessional team communication.